Concept explainers
Videos
In humans, hemophilia A (OMIM 306700) is an X-linked recessive disorder that affects the gene for factor VIII protein, which is essential for blood clotting. The dominant and recessive alleles for the factor VIII gene are represented by H and h. Albinism is an autosomal recessive condition that results from mutation of the gene producing tyrosinase, an enzyme in the melanin synthesis pathway. A and a represent the tyrosinase alleles. A healthy woman named Clara (II-2), whose father (I-1) has hemophilia and whose brother (II-1) has albinism, is married to a healthy man named Charles (II-3), whose parents are healthy. Charles’s brother (II-5) has hemophilia, and his sister (II-4) has albinism. The pedigree is shown below.
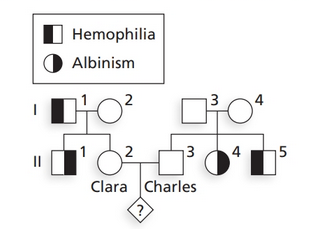
a. What are the genotypes of the four parents (I-1 to I-4) in this pedigree?
b. Determine the probability that the first child of Clara and Charles will be a
i. boy with hemophilia
ii. girl with albinism
iii. healthy girl
iv. boy with both albinism and hemophilia
v. boy with albinism
vi. girl with hemophilia
c. If Clara and Charles’s first child has albinism, what is the chance the second child has albinism? Explain why this probability is higher than the probability you calculated in part (b).

Learn your wayIncludes step-by-step video

Chapter 3 Solutions
Genetic Analysis: An Integrated Approach (3rd Edition)
Additional Science Textbook Solutions
Anatomy & Physiology
Campbell Essential Biology with Physiology (6th Edition)
Campbell Essential Biology (6th Edition) - standalone book
Campbell Biology in Focus (2nd Edition)
Anatomy & Physiology (6th Edition)
Microbiology with Diseases by Body System (5th Edition)


- Familial retinoblastoma, a rare autosomal dominant defect, arose in a large family that had no prior history of the disease. Consider the following pedigree (the darkly colored symbols represent affected individuals): a. Circle the individual(s) in which the mutation most likely occurred. b. Is the person who is the source of the mutation affected by retinoblastoma? Justify your answer. c. Assuming that the mutant allele is fully penetrant, what is the chance that an affected individual will have an affected child?arrow_forwardA couple was referred for genetic counseling because they wanted to know the chances of having a child with dwarfism. Both the man and the woman had achondroplasia (MIM 100800), the most common form of short-limbed dwarfism. The couple knew that this condition is inherited as an autosomal dominant trait, but they were unsure what kind of physical manifestations a child would have if it inherited both mutant alleles. They were each heterozygous for the FGFR3 (MIM 134934) allele that causes achondroplasia. Normally, the protein encoded by this gene interacts with growth factors outside the cell and receives signals that control growth and development. In achrodroplasia, a mutation alters the activity of the receptor, resulting in a characteristic form of dwarfism. Because both the normal and mutant forms of the FGFR3 protein act before birth, no treatment for achrondroplasia is available. The parents each carry one normal allele and one mutant allele of FGRF3, and they wanted information on their chances of having a homozygous child. The counsellor briefly reviewed the phenotypic features of individuals with achondroplasia. These include facial features (large head with prominent forehead; small, flat nasal bridge; and prominent jaw), very short stature, and shortening of the arms and legs. Physical examination and skeletal X-ray films are used to diagnose this condition. Final adult height is approximately 4 feet. Because achondroplasia is an autosomal dominant condition, a heterozygote has a 1-in-2, or 50%, chance of passing this trait to his or her offspring. However, about 75% of those with achondroplasia have parents of average size who do not carry the mutant allele. In these cases, achondroplasia is due to a new mutation. In the couple being counseled, each individual is heterozygous, and they are at risk for having a homozygous child with two copies of the mutated gene. Infants with homozygous achondroplasia are either stillborn or die shortly after birth. The counselor recommended prenatal diagnosis via ultrasounds at various stages of development. In addition, a DNA test is available to detect the homozygous condition prenatally. What if the couple wanted prenatal testing so that a normal fetus could be aborted?arrow_forwardA couple was referred for genetic counseling because they wanted to know the chances of having a child with dwarfism. Both the man and the woman had achondroplasia (MIM 100800), the most common form of short-limbed dwarfism. The couple knew that this condition is inherited as an autosomal dominant trait, but they were unsure what kind of physical manifestations a child would have if it inherited both mutant alleles. They were each heterozygous for the FGFR3 (MIM 134934) allele that causes achondroplasia. Normally, the protein encoded by this gene interacts with growth factors outside the cell and receives signals that control growth and development. In achrodroplasia, a mutation alters the activity of the receptor, resulting in a characteristic form of dwarfism. Because both the normal and mutant forms of the FGFR3 protein act before birth, no treatment for achrondroplasia is available. The parents each carry one normal allele and one mutant allele of FGRF3, and they wanted information on their chances of having a homozygous child. The counsellor briefly reviewed the phenotypic features of individuals with achondroplasia. These include facial features (large head with prominent forehead; small, flat nasal bridge; and prominent jaw), very short stature, and shortening of the arms and legs. Physical examination and skeletal X-ray films are used to diagnose this condition. Final adult height is approximately 4 feet. Because achondroplasia is an autosomal dominant condition, a heterozygote has a 1-in-2, or 50%, chance of passing this trait to his or her offspring. However, about 75% of those with achondroplasia have parents of average size who do not carry the mutant allele. In these cases, achondroplasia is due to a new mutation. In the couple being counseled, each individual is heterozygous, and they are at risk for having a homozygous child with two copies of the mutated gene. Infants with homozygous achondroplasia are either stillborn or die shortly after birth. The counselor recommended prenatal diagnosis via ultrasounds at various stages of development. In addition, a DNA test is available to detect the homozygous condition prenatally. What is the chance that this couple will have a child with two copies of the dominant mutant gene? What is the chance that the child will have normal height?arrow_forward
- A couple was referred for genetic counseling because they wanted to know the chances of having a child with dwarfism. Both the man and the woman had achondroplasia (MIM 100800), the most common form of short-limbed dwarfism. The couple knew that this condition is inherited as an autosomal dominant trait, but they were unsure what kind of physical manifestations a child would have if it inherited both mutant alleles. They were each heterozygous for the FGFR3 (MIM 134934) allele that causes achondroplasia. Normally, the protein encoded by this gene interacts with growth factors outside the cell and receives signals that control growth and development. In achrodroplasia, a mutation alters the activity of the receptor, resulting in a characteristic form of dwarfism. Because both the normal and mutant forms of the FGFR3 protein act before birth, no treatment for achrondroplasia is available. The parents each carry one normal allele and one mutant allele of FGRF3, and they wanted information on their chances of having a homozygous child. The counsellor briefly reviewed the phenotypic features of individuals with achondroplasia. These include facial features (large head with prominent forehead; small, flat nasal bridge; and prominent jaw), very short stature, and shortening of the arms and legs. Physical examination and skeletal X-ray films are used to diagnose this condition. Final adult height is approximately 4 feet. Because achondroplasia is an autosomal dominant condition, a heterozygote has a 1-in-2, or 50%, chance of passing this trait to his or her offspring. However, about 75% of those with achondroplasia have parents of average size who do not carry the mutant allele. In these cases, achondroplasia is due to a new mutation. In the couple being counseled, each individual is heterozygous, and they are at risk for having a homozygous child with two copies of the mutated gene. Infants with homozygous achondroplasia are either stillborn or die shortly after birth. The counselor recommended prenatal diagnosis via ultrasounds at various stages of development. In addition, a DNA test is available to detect the homozygous condition prenatally. Should the parents be concerned about the heterozygous condition as well as the homozygous mutant condition?arrow_forwardHemophilia A is caused by a recessive X-linked allele that encodes a defective form of a clotting protein. If a affected father and a mother who is known to not be a carrier have children, what percentage of female offspring will have hemophilia?arrow_forwardTay Sachs is a rare autosomal recessive disorder that causes mental and physical disabilities leading to death in infants. Affected individuals are lacking the enzyme hexosaminidase, causing lipids to build up in the brain.The HEXA gene on chromosome 15 codes for hexosaminidase, and a four base pair insertion in the gene results in an altered reading frame and non-functional enzyme being produced. Individuals who are carriers (heterozygotes) of the Tay-Sachs allele are not affected by the disease but appear to have increased protection against tuberculosis.The incidence of Tay-Sachs disease is much higher among Ashkenazi Jews originating from Eastern Europe than the general population of the United States. About 1 in 3 500 babies of Ashkenazi Jewish heritage are born with Tay-Sachs disease and about 1 in 30 Ashkenazi Jews are carriers compared to about 1 in 320 000 babies born with the disease and about 1 in 300 carriers in the general United States population. Ashkenazi Jews living in…arrow_forward
- Lesch-Nyhan syndrome is due to a mutation in a gene that encodesa protein called hypoxanthine-guanine phosphoribosyltransferase(HPRT). HPRT is an enzyme that functions in purine metabolism.People afflicted with this syndrome have severe neurodegenerationand loss of motor control. The pedigree below contains severalindividuals with Lesch-Nyhan syndrome, shown with blacksymbols. Based on this pedigree, does this syndrome appearto be inherited by an autosomal recessive, autosomal dominant,X-linked recessive, or X-linked dominant pattern? Explainyour reasoning.arrow_forwardTake the example of B-thalassemia, an autosomal recessive genetic disease that particularly affects people from around the Mediterranean. This disease is associated with an anomaly of hemoglobin, a protein essential for the transport of oxygen, which is composed of four chains: two alpha (a) and two beta (B). In case of B-thalassemia, the ẞ chains are produced in insufficient or no quantity in an individual homozygous recessive resulting in insufficient production of overall hemoglobin leading to anemia and other physiological challenges. The gene that controls the synthesis of the ẞ chains is located on chromosome 11. Here is part of the coding portion of this gene (which controls a total of 146 amino acids and of which you only see the portion 36 to 41) and one of the targeted mutations: 1. Give the sequence of amino acids from the template and mutated strands. 2. What type of point mutation is it? 3. Using the principles of the theory of evolution, explain briefly and generally why…arrow_forwardIn humans, ABO blood types refer to glycoproteins in the membranes of red blood cells. There are three alleles for this autosomal gene: IA, IB, and i. The IA allele codes for the A sugar, The IB allele codes for the B sugar, and the i allele doesn't code for any sugar. IA and IB are codominant, and i is recessive to both IA and IB. If an individual with type AB blood has a child with an individual with type O blood, what blood types could their children possibly have?arrow_forward
- The following pedigree illustrates the inheritance of Nance–Horan syndrome, a rare genetic condition in which affected people have cataracts and abnormally shaped teeth.arrow_forwardShown below is a pedigree for Phenylketonuria (PKU), an autosomal recessive metabolic disorder. The characteristic feature of PKU is severe mental retardation A) What is the probability that individual II-1 is heterozygous for this gene? B) What is the probability that individual III-4 is heterozygous for this gene? C) If individuals III-3 and III-4 were to marry, what is the probability that their child would express PKU?arrow_forwardBelow is a pedigree chart for a family that has a history of Alkaptonuria. Individuals infected with this condition can have darkened skin, brown urine, and can suffer from joint damage and other complications. Given this pedigree answer the following questions. Given the data in the pedigree chart is this genetic condition autosomal dominant or autosomal recessive? What are the genotypes for #1, #2, and #3? If either of the 4th generation "aa" females were to mate with a homozygous dominant male would any of their offspring illustrate the phenotype? Why or why not?arrow_forward
 Human Heredity: Principles and Issues (MindTap Co...BiologyISBN:9781305251052Author:Michael CummingsPublisher:Cengage Learning
Human Heredity: Principles and Issues (MindTap Co...BiologyISBN:9781305251052Author:Michael CummingsPublisher:Cengage Learning Biology Today and Tomorrow without Physiology (Mi...BiologyISBN:9781305117396Author:Cecie Starr, Christine Evers, Lisa StarrPublisher:Cengage Learning
Biology Today and Tomorrow without Physiology (Mi...BiologyISBN:9781305117396Author:Cecie Starr, Christine Evers, Lisa StarrPublisher:Cengage Learning