. What nursing assessment findings support the diagnosis of Liver Cirrhosis? 2. Correlate the patient’s presenting clinical manifestations of esophageal varices in liver cirrhosis? 3. In what order should the nurse institute the physician orders that are listed above? Perform dosage calculations and state how to administer the medications. 4. The nurse observes the nasogastric secretions and, upon admission to the ICU, there was 200 mL of dark red-colored drainage. The nurse continues to monitor the drainage and, as the nurse hangs the first unit of PRBCs, 200 mL of bright red bloody drainage is dumped into the collection canister. What should the nurse do? 5. The gastroenterologist orders for the nu
. What nursing assessment findings support the diagnosis of Liver Cirrhosis? 2. Correlate the patient’s presenting clinical manifestations of esophageal varices in liver cirrhosis? 3. In what order should the nurse institute the physician orders that are listed above? Perform dosage calculations and state how to administer the medications. 4. The nurse observes the nasogastric secretions and, upon admission to the ICU, there was 200 mL of dark red-colored drainage. The nurse continues to monitor the drainage and, as the nurse hangs the first unit of PRBCs, 200 mL of bright red bloody drainage is dumped into the collection canister. What should the nurse do? 5. The gastroenterologist orders for the nu
. What nursing assessment findings support the diagnosis of Liver Cirrhosis? 2. Correlate the patient’s presenting clinical manifestations of esophageal varices in liver cirrhosis? 3. In what order should the nurse institute the physician orders that are listed above? Perform dosage calculations and state how to administer the medications. 4. The nurse observes the nasogastric secretions and, upon admission to the ICU, there was 200 mL of dark red-colored drainage. The nurse continues to monitor the drainage and, as the nurse hangs the first unit of PRBCs, 200 mL of bright red bloody drainage is dumped into the collection canister. What should the nurse do? 5. The gastroenterologist orders for the nu
1. What nursing assessment findings support the diagnosis of Liver Cirrhosis?
2. Correlate the patient’s presenting clinical manifestations of esophageal varices in liver cirrhosis?
3. In what order should the nurse institute the physician orders that are listed above? Perform dosage calculations and state how to administer the medications.
4. The nurse observes the nasogastric secretions and, upon admission to the ICU, there was 200 mL of dark red-colored drainage. The nurse continues to monitor the drainage and, as the nurse hangs the first unit of PRBCs, 200 mL of bright red bloody drainage is dumped into the collection canister. What should the nurse do?
5. The gastroenterologist orders for the nurse to increase the octreotide to 50 mcg/hr and the endoscopy nurse and the physician will be up shortly to perform a vertical band ligation (VBL). What does the nurse need to do in preparation for this procedure?
6. What nursing diagnoses should the nurse formulate for the patient?
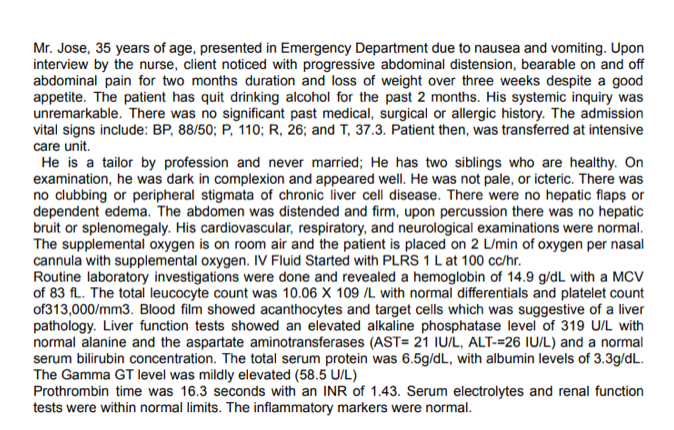
Transcribed Image Text:Mr. Jose, 35 years of age, presented in Emergency Department due to nausea and vomiting. Upon
interview by the nurse, client noticed with progressive abdominal distension, bearable on and off
abdominal pain for two months duration and loss of weight over three weeks despite a good
appetite. The patient has quit drinking alcohol for the past 2 months. His systemic inquiry was
unremarkable. There was no significant past medical, surgical or allergic history. The admission
vital signs include: BP, 88/50; P, 110; R, 26; and T, 37.3. Patient then, was transferred at intensive
care unit.
He is a tailor by profession and never married; He has two siblings who are healthy. On
examination, he was dark in complexion and appeared well. He was not pale, or icteric. There was
no clubbing or peripheral stigmata of chronic liver cell disease. There were no hepatic flaps or
dependent edema. The abdomen was distended and firm, upon percussion there was no hepatic
bruit or splenomegaly. His cardiovascular, respiratory, and neurological examinations were normal.
The supplemental oxygen is on room air and the patient is placed on 2 L/min of oxygen per nasal
cannula with supplemental oxygen. IV Fluid Started with PLRS 1 Lat 100 cc/hr.
Routine laboratory investigations were done and revealed a hemoglobin of 14.9 g/dL with a MCV
of 83 fL. The total leucocyte count was 10.06 X 109 /L with normal differentials and platelet count
of313,000/mm3. Blood film showed acanthocytes and target cells which was suggestive of a liver
pathology. Liver function tests showed an elevated alkaline phosphatase level of 319 U/L with
normal alanine and the aspartate aminotransferases (AST= 21 IU/L, ALT-=26 IU/L) and a normal
serum bilirubin concentration. The total serum protein was 6.5g/dL, with albumin levels of 3.3g/dL.
The Gamma GT level was mildly elevated (58.5 U/L)
Prothrombin time was 16.3 seconds with an INR of 1.43. Serum electrolytes and renal function
tests were within normal limits. The inflammatory markers were normal.
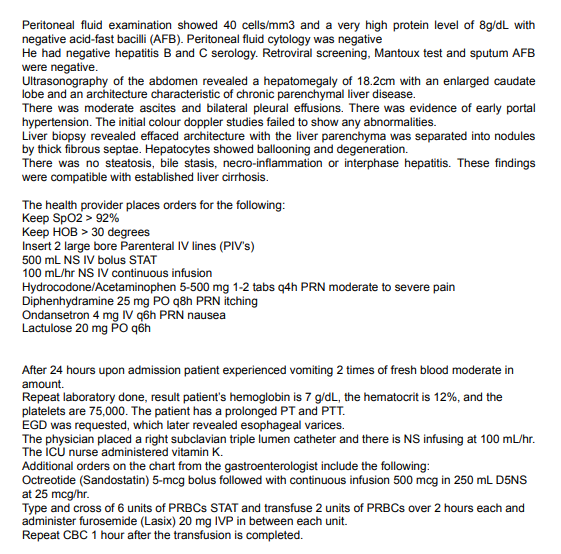
Transcribed Image Text:Peritoneal fluid examination showed 40 cells/mm3 and a very high protein level of 8g/dL with
negative acid-fast bacilli (AFB). Peritoneal fluid cytology was negative
He had negative hepatitis B and C serology. Retroviral screening, Mantoux test and sputum AFB
were negative.
Ultrasonography of the abdomen revealed a hepatomegaly of 18.2cm with an enlarged caudate
lobe and an architecture characteristic of chronic parenchymal liver disease.
There was moderate ascites and bilateral pleural effusions. There was evidence of early portal
hypertension. The initial colour doppler studies failed to show any abnormalities.
Liver biopsy revealed effaced architecture with the liver parenchyma was separated into nodules
by thick fibrous septae. Hepatocytes showed ballooning and degeneration.
There was no steatosis, bile stasis, necro-inflammation or interphase hepatitis. These findings
were compatible with established liver cirrhosis.
The health provider places orders for the following:
Kеep Spo2> 92%
Keep HOB > 30 degrees
Insert 2 large bore Parenteral IV lines (PIV's)
500 mL NS IV bolus STAT
100 mL/hr NS IV continuous infusion
Hydrocodone/Acetaminophen 5-500 mg 1-2 tabs q4h PRN moderate to severe pain
Diphenhydramine 25 mg PO q8h PRN itching
Ondansetron 4 mg IV q6h PRN nausea
Lactulose 20 mg PO qồh
After 24 hours upon admission patient experienced vomiting 2 times of fresh blood moderate in
amount.
Repeat laboratory done, result patient's hemoglobin is 7 g/dL, the hematocrit is 12%, and the
platelets are 75,000. The patient has a prolonged PT and PTT.
EGD was requested, which later revealed esophageal varices.
The physician placed a right subclavian triple lumen catheter and there is NS infusing at 100 mL/hr.
The iCú nurse administered vitamin K.
Additional orders on the chart from the gastroenterologist include the following:
Octreotide (Sandostatin) 5-mcg bolus followed with continuous infusion 500 mcg in 250 mL D5NS
at 25 mcg/hr.
Type and cross of 6 units of PRBCS STAT and transfuse 2 units of PRBCS over 2 hours each and
administer furosemide (Lasix) 20 mg IVP in between each unit.
Repeat CBC 1 hour after the transfusion is completed.
Expert Solution
This question has been solved!
Explore an expertly crafted, step-by-step solution for a thorough understanding of key concepts.