CASE STUDY A 65-year-old man with a 60-pack-year history of cigarette smoking presents with worsening exertional dyspnea. Pulmonary function testing showed significant restrictive lung disease that was thought to be secondary to the patient's chronic obstructive pulmonary disease (COPD). Two-dimensional echocardiography revealed a mean pulmonary artery pressure (PAP) of 53 mm Hg with normal right ventricular size and function. Right heart catheterization at the time of diagnosis confirmed the elevated mean PAP with a capillary wedge pressure of 12 mm Hg and peripheral vascular resistance of 7 wood units. The study was positive for vasodilator response with a drop in mean PAP to 40 mm Hg. Cardiac output remained stable. The patient was started on long-acting nifedipine. Ventilation perfusion scan showed no mismatched perfusion defects. Complete metabolic profile and complete blood count were normal, and screening for HIV was negative. High- resolution CT of the lungs showed evidence of pulmonary fibrosis. The patient was given a diagnosis of concomitant idiopathic pulmonary fibrosis and COPD. Initially, he appeared to do well with the nifedipine with improved symptoms but presented back for evaluation 2 months later with worsening shortness of breath with minimal activity. He feels well at rest but gets markedly short of breath when washing dishes or walking to the bathroom. He is medically optimized for his COPD, with multiple inhaled medications and inhaled corticosteroids. Physical exam revealed 1+ bilateral lower extremity edema and hepatomegaly. Cardiovascular exam revealed a right ventricular heave, jugular venous distention to his jaw, and lungs that are clear to auscultation. Follow-up labs revealed a N-terminal pro-B- type natriuretic peptide level of 500 pg/mL, and a repeat 2-dimensional echo revealed mild right atrial dilatation, trace pericardial effusion, and a dilated inferior vena cava with partial collapse. Left ventricular function remained reserved Right ventricular systolic pressure is calculated at 55 mm Hg. The patients is sent for a repeat right heart catheterization, which confirms the elevated mean PAP of 50 mm Hg. His cardiac index is calculated to be 2.0 Liminute/m?. According to the World Health Organization classification for pulmonary hypertension, he is at functional class (WHO- FC) III. Finally, he is referred for cardiopulmonary testing and is found to have a peak VOz of 14 mL/minute/kg.
CASE STUDY A 65-year-old man with a 60-pack-year history of cigarette smoking presents with worsening exertional dyspnea. Pulmonary function testing showed significant restrictive lung disease that was thought to be secondary to the patient's chronic obstructive pulmonary disease (COPD). Two-dimensional echocardiography revealed a mean pulmonary artery pressure (PAP) of 53 mm Hg with normal right ventricular size and function. Right heart catheterization at the time of diagnosis confirmed the elevated mean PAP with a capillary wedge pressure of 12 mm Hg and peripheral vascular resistance of 7 wood units. The study was positive for vasodilator response with a drop in mean PAP to 40 mm Hg. Cardiac output remained stable. The patient was started on long-acting nifedipine. Ventilation perfusion scan showed no mismatched perfusion defects. Complete metabolic profile and complete blood count were normal, and screening for HIV was negative. High- resolution CT of the lungs showed evidence of pulmonary fibrosis. The patient was given a diagnosis of concomitant idiopathic pulmonary fibrosis and COPD. Initially, he appeared to do well with the nifedipine with improved symptoms but presented back for evaluation 2 months later with worsening shortness of breath with minimal activity. He feels well at rest but gets markedly short of breath when washing dishes or walking to the bathroom. He is medically optimized for his COPD, with multiple inhaled medications and inhaled corticosteroids. Physical exam revealed 1+ bilateral lower extremity edema and hepatomegaly. Cardiovascular exam revealed a right ventricular heave, jugular venous distention to his jaw, and lungs that are clear to auscultation. Follow-up labs revealed a N-terminal pro-B- type natriuretic peptide level of 500 pg/mL, and a repeat 2-dimensional echo revealed mild right atrial dilatation, trace pericardial effusion, and a dilated inferior vena cava with partial collapse. Left ventricular function remained reserved Right ventricular systolic pressure is calculated at 55 mm Hg. The patients is sent for a repeat right heart catheterization, which confirms the elevated mean PAP of 50 mm Hg. His cardiac index is calculated to be 2.0 Liminute/m?. According to the World Health Organization classification for pulmonary hypertension, he is at functional class (WHO- FC) III. Finally, he is referred for cardiopulmonary testing and is found to have a peak VOz of 14 mL/minute/kg.

Surgical Tech For Surgical Tech Pos Care
5th Edition
ISBN:9781337648868
Author:Association
Publisher:Association
Chapter9: Surgical Pharmacology And Anesthesia
Section: Chapter Questions
Problem 3CS

Related questions
Question
make a ncp
Assessment
Nursing diagnosis
Planning
Intervention
Evaluation
Transcribed Image Text:CASE STUDY
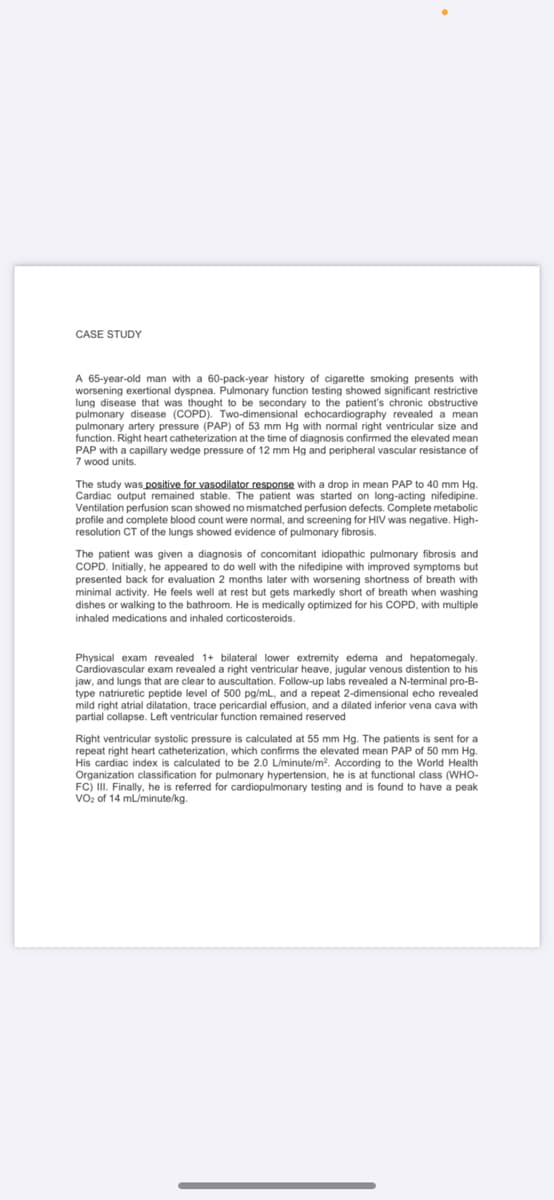
A 65-year-old man with a 60-pack-year history of cigarette smoking presents with
worsening exertional dyspnea. Pulmonary function testing showed significant restrictive
lung disease that was thought to be secondary to the patient's chronic obstructive
pulmonary disease (COPD). Two-dimensional echocardiography revealed a mean
pulmonary artery pressure (PAP) of 53 mm Hg with normal right ventricular size and
function. Right heart catheterization at the time of diagnosis confirmed the elevated mean
PAP with a capillary wedge pressure of 12 mm Hg and peripheral vascular resistance of
7 wood units.
The study was positive for vasodilator response with a drop in mean PAP to 40 mm Hg.
Cardiac output remained stable. The patient was started on long-acting nifedipine.
Ventilation perfusion scan showed no mismatched perfusion defects. Complete metabolic
profile and complete blood count were normal, and screening for HIV was negative. High-
resolution CT of the lungs showed evidence of pulmonary fibrosis.
The patient was given a diagnosis of concomitant idiopathic pulmonary fibrosis and
COPD. Initially, he appeared to do well with the nifedipine with improved symptoms but
presented back for evaluation 2 months later with worsening shortness of breath with
minimal activity. He feels well at rest but gets markedly short of breath when washing
dishes or walking to the bathroom. He is medically optimized for his COPD, with multiple
inhaled medications and inhaled corticosteroids.
Physical exam revealed 1+ bilateral lower extremity edema and hepatomegaly.
Cardiovascular exam revealed a right ventricular heave, jugular venous distention to his
jaw, and lungs that are clear to auscultation. Follow-up labs revealed a N-terminal pro-B-
type natriuretic peptide level of 500 pg/mL, and a repeat 2-dimensional echo revealed
mild right atrial dilatation, trace pericardial effusion, and a dilated inferior vena cava with
partial collapse. Left ventricular function remained reserved
Right ventricular systolic pressure is calculated at 55 mm Hg. The patients is sent fo
repeat right heart catheterization, which confirms the elevated mean PAP of 50 mm Hg.
His cardiac index is calculated to be 2.0 L/minute/m2. According to the World Health
Organization classification for pulmonary hypertension, he is at functional class (WHO-
FC) II. Finally, he is referred for cardiopulmonary testing and is found to have a peak
of 14 mL/minute/kg.
Vo2
Expert Solution
This question has been solved!
Explore an expertly crafted, step-by-step solution for a thorough understanding of key concepts.

This is a popular solution!

Trending now
This is a popular solution!

Step by step
Solved in 6 steps

Knowledge Booster


Learn more about
Need a deep-dive on the concept behind this application? Look no further. Learn more about this topic, nursing and related others by exploring similar questions and additional content below.Recommended textbooks for you
Surgical Tech For Surgical Tech Pos Care
Health & Nutrition
ISBN:
9781337648868
Author:
Association
Publisher:
Cengage
Basic Clinical Lab Competencies for Respiratory C…
Nursing
ISBN:
9781285244662
Author:
White
Publisher:
Cengage
Surgical Tech For Surgical Tech Pos Care
Health & Nutrition
ISBN:
9781337648868
Author:
Association
Publisher:
Cengage
Basic Clinical Lab Competencies for Respiratory C…
Nursing
ISBN:
9781285244662
Author:
White
Publisher:
Cengage