
Surgical Tech For Surgical Tech Pos Care
5th Edition
ISBN:9781337648868
Author:Association
Publisher:Association
Chapter7: Preventing Perioperative Disease Transmission
Section: Chapter Questions
Problem 7.2.4CS

Related questions
Question
make a nursing care plan
Transcribed Image Text:CASE STUDY
Peripheral Arterial Disease: A Case Report
From the Henry Ford Hospital
Shel D. Levine, MS, ACSM-CEP'
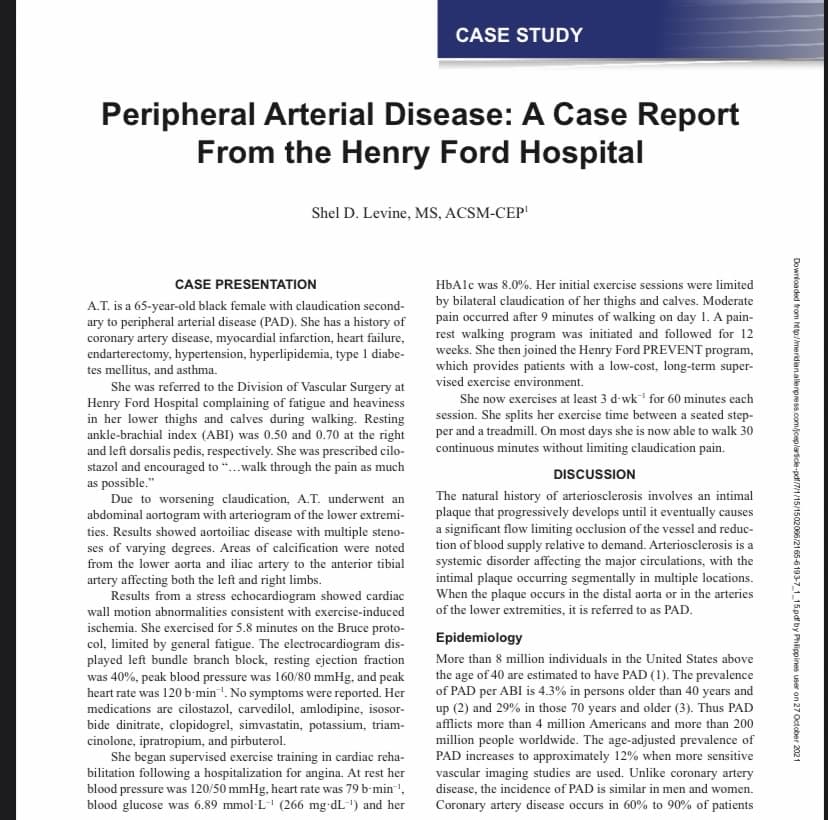
CASE PRESENTATION
HbAlc was 8.0%. Her initial exercise sessions were limited
A.T. is a 65-year-old black female with claudication second-
ary to peripheral arterial disease (PAD). She has a history of
coronary artery disease, myocardial infarction, heart failure,
endarterectomy, hypertension, hyperlipidemia, type 1 diabe-
tes mellitus, and asthma.
by bilateral claudication of her thighs and calves. Moderate
pain occurred after 9 minutes of walking on day 1. A pain-
rest walking program was initiated and followed for 12
weeks. She then joined the Henry Ford PREVENT program,
which provides patients with a low-cost, long-term super-
vised exercise environment.
She was referred to the Division of Vascular Surgery at
Henry Ford Hospital complaining of fatigue and heaviness
in her lower thighs and calves during walking. Resting
ankle-brachial index (ABI) was 0.50 and 0.70 at the right
and left dorsalis pedis, respectively. She was prescribed cilo-
stazol and encouraged to “.walk through the pain as much
as possible."
Due to worsening claudication, A.T. underwent an
abdominal aortogram with arteriogram of the lower extremi-
ties. Results showed aortoiliac disease with multiple steno-
ses of varying degrees. Areas of calcification were noted
from the lower aorta and iliac artery to the anterior tibial
artery affecting both the left and right limbs.
Results from a stress echocardiogram showed cardiac
She now exercises at least 3 d-wk for 60 minutes each
session. She splits her exercise time between a seated step-
per and a treadmill. On most days she is now able to walk 30
continuous minutes without limiting claudication pain.
DISCUSSION
The natural history of arteriosclerosis involves an intimal
plaque that progressively develops until it eventually causes
a significant flow limiting occlusion of the vessel and reduc-
tion of blood supply relative to demand. Arteriosclerosis is a
systemic disorder affecting the major circulations, with the
intimal plaque occurring segmentally in multiple locations.
When the plaque occurs in the distal aorta or in the arteries
of the lower extremities, it is referred to as PAD.
wall motion abnormalities consistent with exercise-induced
ischemia. She exercised for 5.8 minutes on the Bruce proto-
col, limited by general fatigue. The electrocardiogram dis-
played left bundle branch block, resting ejection fraction
was 40%, peak blood pressure was 160/80 mmHg, and peak
heart rate was 120 b'min'. No symptoms were reported. Her
medications are cilostazol, carvedilol, amlodipine, isosor-
bide dinitrate, clopidogrel, simvastatin, potassium, triam-
cinolone, ipratropium, and pirbuterol.
She began supervised exercise training in cardiac reha-
bilitation following a hospitalization for angina. At rest her
blood pressure was 120/50 mmHg, heart rate was 79 b-min',
blood glucose was 6.89 mmol-L" (266 mg-dL-") and her
Epidemiology
More than 8 million individuals in the United States above
the age of 40 are estimated to have PAD (1). The prevalence
of PAD per ABI is 4.3% in persons older than 40 years and
up (2) and 29% in those 70 years and older (3). Thus PAD
afflicts more than 4 million Americans and more than 200
million people worldwide. The age-adjusted prevalence of
PAD increases to approximately 12% when more sensitive
vascular imaging studies are used. Unlike coronary artery
disease, the incidence of PAD is similar in men and women.
Coronary artery disease occurs in 60% to 90% of patients
Downloaded from http:/meridian.allerpress.com/jceplartice-pdf/7/1/15/1502066/2165-6193-7_115pdf by Phlippines user on 27 October 2021
Expert Solution
This question has been solved!
Explore an expertly crafted, step-by-step solution for a thorough understanding of key concepts.

This is a popular solution!

Trending now
This is a popular solution!

Step by step
Solved in 2 steps

Recommended textbooks for you
Surgical Tech For Surgical Tech Pos Care
Health & Nutrition
ISBN:
9781337648868
Author:
Association
Publisher:
Cengage
Basic Clinical Lab Competencies for Respiratory C…
Nursing
ISBN:
9781285244662
Author:
White
Publisher:
Cengage
Surgical Tech For Surgical Tech Pos Care
Health & Nutrition
ISBN:
9781337648868
Author:
Association
Publisher:
Cengage
Basic Clinical Lab Competencies for Respiratory C…
Nursing
ISBN:
9781285244662
Author:
White
Publisher:
Cengage