
Chapter14: Allergy: An Overview
Section: Chapter Questions
Problem 21RQ

Related questions
Question
nursing care plan
Transcribed Image Text:9:05
ull ?
Done
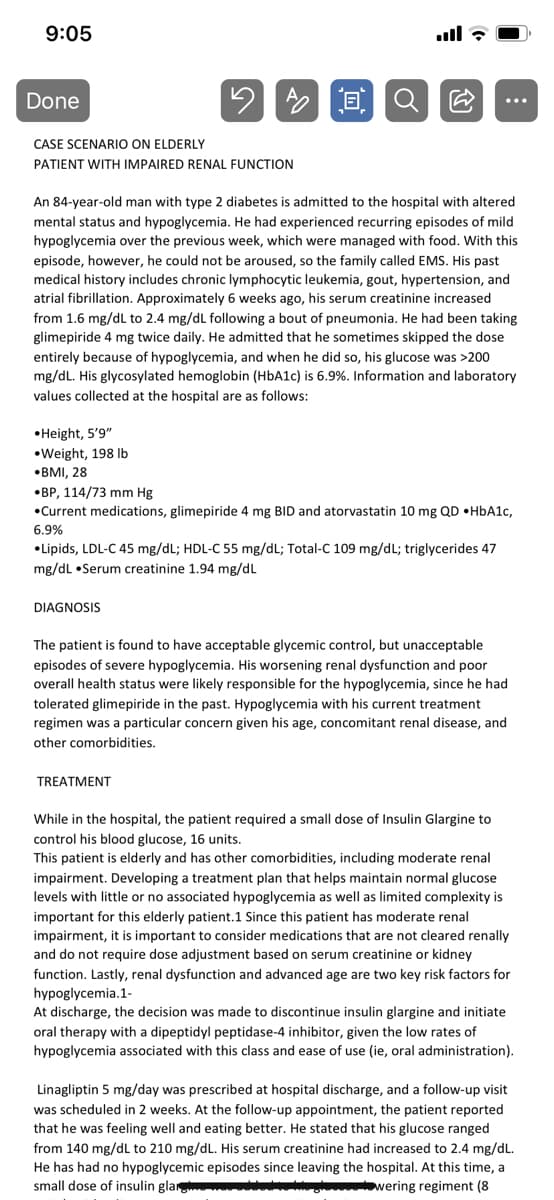
CASE SCENARIO ON ELDERLY
PATIENT WITH IMPAIRED RENAL FUNCTION
An 84-year-old man with type 2 diabetes is admitted to the hospital with altered
mental status and hypoglycemia. He had experienced recurring episodes of mild
hypoglycemia over the previous week, which were managed with food. With this
episode, however, he could not be aroused, so the family called EMS. His past
medical history includes chronic lymphocytic leukemia, gout, hypertension, and
atrial fibrillation. Approximately 6 weeks ago, his serum creatinine increased
from 1.6 mg/dL to 2.4 mg/dL following a bout of pneumonia. He had been taking
glimepiride 4 mg twice daily. He admitted that he sometimes skipped the dose
entirely because of hypoglycemia, and when he did so, his glucose was >200
mg/dL. His glycosylated hemoglobin (HbA1c) is 6.9%. Information and laboratory
values collected at the hospital are as follows:
•Height, 5'9"
•Weight, 198 Ib
•BMI, 28
•BP, 114/73 mm Hg
•Current medications, glimepiride 4 mg BID and atorvastatin 10 mg QD •HBA1C,
6.9%
• Lipids, LDL-C 45 mg/dL; HDL-C 55 mg/dL; Total-C 109 mg/dL; triglycerides 47
mg/dL •Serum creatinine 1.94 mg/dL
DIAGNOSIS
The patient is found to have acceptable glycemic control, but unacceptable
episodes of severe hypoglycemia. His worsening renal dysfunction and poor
overall health status were likely responsible for the hypoglycemia, since he had
tolerated glimepiride in the past. Hypoglycemia with his current treatment
regimen was a particular concern given his age, concomitant renal disease, and
other comorbidities.
TREATMENT
While in the hospital, the patient required a small dose of Insulin Glargine to
control his blood glucose, 16 units.
This patient is elderly and has other comorbidities, including moderate renal
impairment. Developing a treatment plan that helps maintain normal glucose
levels with little or no associated hypoglycemia as well as limited complexity is
important for this elderly patient.1 Since this patient has moderate renal
impairment, it is important to consider medications that are not cleared renally
and do not require dose adjustment based on serum creatinine or kidney
function. Lastly, renal dysfunction and advanced age are two key risk factors for
hypoglycemia.1-
At discharge, the decision was made to discontinue insulin glargine and initiate
oral therapy with a dipeptidyl peptidase-4 inhibitor, given the low rates of
hypoglycemia associated with this class and ease of use (ie, oral administration).
Linagliptin 5 mg/day was prescribed at hospital discharge, and a follow-up visit
was scheduled in 2 weeks. At the follow-up appointment, the patient reported
that he was feeling well and eating better. He stated that his glucose ranged
from 140 mg/dL to 210 mg/dL. His serum creatinine had increased to 2.4 mg/dL.
He has had no hypoglycemic episodes since leaving the hospital. At this time, a
small dose of insulin gla
wering regiment (8
Transcribed Image Text:9:05
ull ?
•Lipids, LDL-C 45 mg/dL; HDL-C 55 mg/dL; Total-C 109 mg/dL; triglycerides 47
mg/dL •Serum creatinine 1.94 mg/dL
DIAGNOSIS
The patient is found to have acceptable glycemic control, but unacceptable
episodes of severe hypoglycemia. His worsening renal dysfunction and poor
overall health status were likely responsible for the hypoglycemia, since he had
tolerated glimepiride in the past. Hypoglycemia with his current treatment
regimen was a particular concern given his age, concomitant renal disease, and
other comorbidities.
TREATMENT
While in the hospital, the patient required a small dose of Insulin Glargine to
control his blood glucose, 16 units.
This patient is elderly and has other comorbidities, including moderate renal
impairment. Developing a treatment plan that helps maintain normal glucose
levels with little or no associated hypoglycemia as well as limited complexity is
important for this elderly patient.1 Since this patient has moderate renal
impairment, it is important to consider medications that are not cleared renally
and do not require dose adjustment based on serum creatinine or kidney
function. Lastly, renal dysfunction and advanced age are two key risk factors for
hypoglycemia.1-
At discharge, the decision was made to discontinue insulin glargine and initiate
oral therapy with a dipeptidyl peptidase-4 inhibitor, given the low rates of
hypoglycemia associated with this class and ease of use (ie, oral administration).
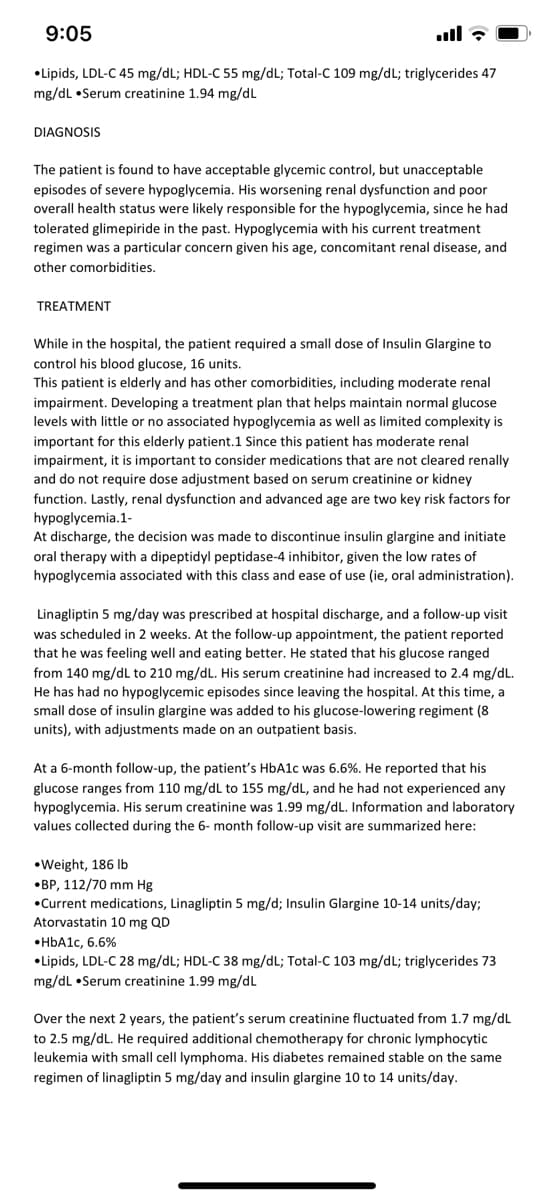
Linagliptin 5 mg/day was prescribed at hospital discharge, and a follow-up visit
was scheduled in 2 weeks. At the follow-up appointment, the patient reported
that he was feeling well and eating better. He stated that his glucose ranged
from 140 mg/dL to 210 mg/dL. His serum creatinine had increased to 2.4 mg/dL.
He has had no hypoglycemic episodes since leaving the hospital. At this time, a
small dose of insulin glargine was added to his glucose-lowering regiment (8
units), with adjustments made on an outpatient basis.
At a 6-month follow-up, the patient's HbA1c was 6.6%. He reported that his
glucose ranges from 110 mg/dL to 155 mg/dL, and he had not experienced any
hypoglycemia. His serum creatinine was 1.99 mg/dL. Information and laboratory
values collected during the 6- month follow-up visit are summarized here:
•Weight, 186 Ib
•BP, 112/70 mm Hg
•Current medications, Linagliptin 5 mg/d; Insulin Glargine 10-14 units/day;
Atorvastatin 10 mg QD
•HBA1C, 6.6%
•Lipids, LDL-C 28 mg/dL; HDL-C 38 mg/dL; Total-C 103 mg/dL; triglycerides 73
mg/dL •Serum creatinine 1.99 mg/dL
Over the next 2 years, the patient's serum creatinine fluctuated from 1.7 mg/dL
to 2.5 mg/dL. He required additional chemotherapy for chronic lymphocytic
leukemia with small cell lymphoma. His diabetes remained stable on the same
regimen of linagliptin 5 mg/day and insulin glargine 10 to 14 units/day.
Expert Solution
This question has been solved!
Explore an expertly crafted, step-by-step solution for a thorough understanding of key concepts.

This is a popular solution!

Trending now
This is a popular solution!

Step by step
Solved in 3 steps

Recommended textbooks for you
Essentials of Pharmacology for Health Professions
Nursing
ISBN:
9781305441620
Author:
WOODROW
Publisher:
Cengage