Why should medications other than glipizide or glyburide be considered for management of diabetes in this patient? List four sighs of dehydration in this patient? What is the significance of xerosis and cracking of the feet in this patient?
Why should medications other than glipizide or glyburide be considered for management of diabetes in this patient? List four sighs of dehydration in this patient? What is the significance of xerosis and cracking of the feet in this patient?

Surgical Tech For Surgical Tech Pos Care
5th Edition
ISBN:9781337648868
Author:Association
Publisher:Association
Chapter9: Surgical Pharmacology And Anesthesia
Section: Chapter Questions
Problem 9.3CS

Related questions
Question
Why should medications other than glipizide or glyburide be considered for management of diabetes in this patient?
List four sighs of dehydration in this patient?
What is the significance of xerosis and cracking of the feet in this patient?
Transcribed Image Text:262| PART 7- NEUROENDOCRINE DISORDERS
CASE STUDY 54= DIABETES MELLITUS, TYPE 2 263
Heart
Pa
can
• Regular rate and rhythm with no murmurs, gallops, or rubs
• Apical impulse normal at 5th ICS at mid-clavicular line
• Normal S, ands,
• No S, S,
case
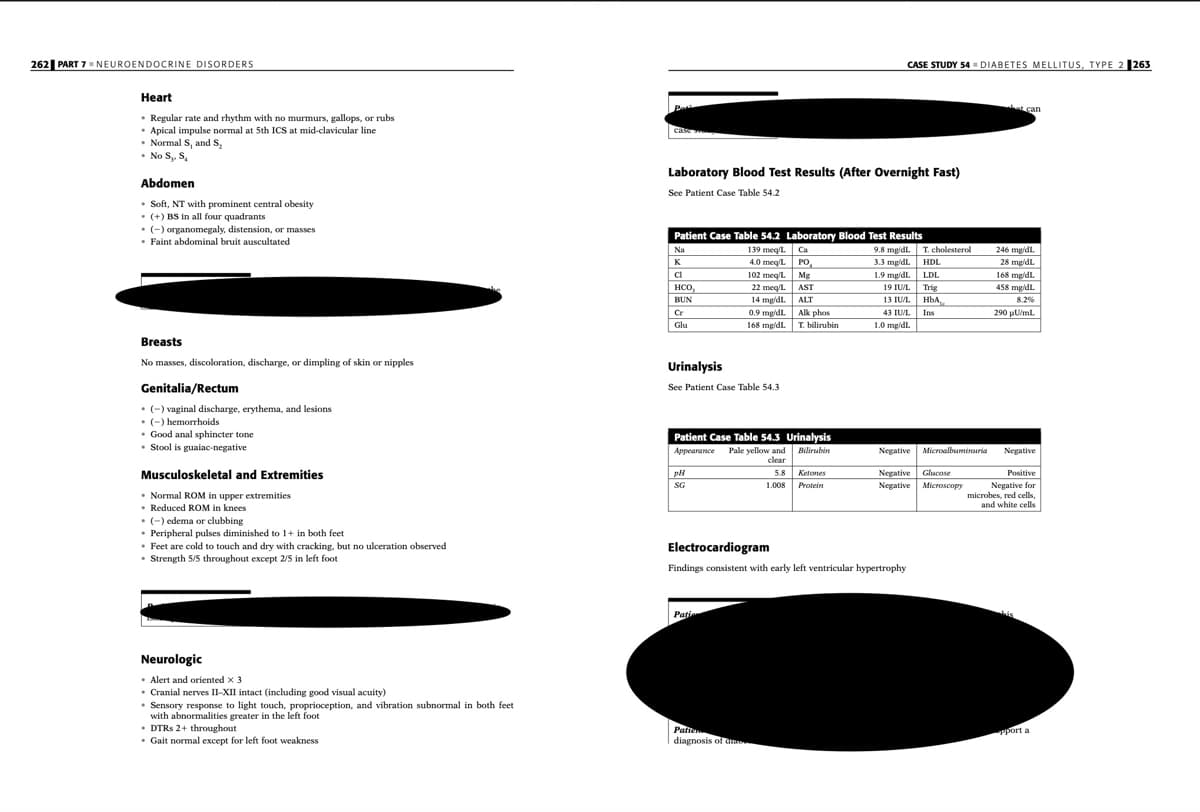
Laboratory Blood Test Results (After Overnight Fast)
Abdomen
See Patient Case Table 54.2
• Soft, NT with prominent central obesity
• (+) BS in all four quadrants
• (-) organomegaly, distension, or masses
• Faint abdominal bruit auscultated
Patient Case Table 54.2 Laboratory Blood Test Results
9.8 mg/dl.
3.3 mg/dL.
1.9 mg/dL LDL
19 IU/L Trig
HbA,
43 IU/L.
139 meg/l. Ca
4.0 meq/L PO,
Na
T. cholesterol
246 mg/dl.
K
HDL
28 mg/dL.
168 mg/dL
ci
102 meg L Mg
22 meq/l. AST
14 mg/dl. ALT
0.9 mg/dl. Alk phos
нсо,
HCO,
458 mgidl.
BUN
13 IUL
8.2%
Cr
Ins
290 uU/ml.
Glu
168 mg/dl. T. bilirubin
1.0 mg/dl.
Breasts
No masses, discoloration, discharge, or dimpling of skin or nipples
Urinalysis
Genitalia/Rectum
See Patient Case Table 54.3
• (-) vaginal discharge, erythema, and lesions
• (-) hemorrhoids
• Good anal sphincter tone
• Stool is guaiac-negative
Patient Case Table 54.3 Urinalysis
Appearance Pale yellow and
clear
Bilirubin
Negative
Microalbuminuria
Negative
Musculoskeletal and Extremities
5.8
Ketones
Negative
Glucose
Positive
Negative for
microbes, red cells,
and white cells
SG
1.008
Protein
Negative Microscopy
• Normal ROM in upper extremities
• Reduced ROM in knees
• (-) edema or clubbing
• Peripheral pulses diminished to 1+ in both feet
• Feet are cold to touch and dry with cracking, but no ulceration observed
• Strength 5/5 throughout except 2/5 in left foot
Electrocardiogram
Findings consistent with early left ventricular hypertrophy
Patie
Neurologic
• Alert and oriented x 3
• Cranial nerves II-XII intact (including good visual acuity)
• Sensory response to light touch, proprioception, and vibration subnormal in both feet
with abnormalities greater in the left foot
• DTRS 2+ throughout
• Gait normal except for left foot weakness
Palte
diagnosis of dn
Pport a
Transcribed Image Text:CASE STUDY 54▪ DIABETES MELLITUS, TYPE 2 259
CASE STUDY
Past Surgical History
54
C-section 14 years ago
DIABETES MELLITUS, TYPE 2
OB-GYN History
• Menarche at age 12
• Menopause, natural, at age 46%: despite problematic hot flashes, she has chosen not to ini-
tiate HRT
• First child at age 17, last child at age 34, G,P,A, all babies were healthy, 4th child weighed
10 Ibs 6% oz at birth
• Last Pap smear 4 years ago
Family History
• Type 2 DM present in younger sister and maternal grandmother; both were diagnosed
in their late 40s; maternal grandmother died from kidney failure while waiting for a kidney
transplant; sister is taking "pills and shots"
• Father had emphysema
• Two older siblings are alive and apparently well
• All four children are healthy
For the Disease Summary for this case study,
see the CD-ROM.
PATIENT CASE
Patient's Chief Complaints
"My left foot feels weak and numb. I have a hard time pointing my toes up."
Social History
• Married 29 years with 4 children; husband is a migrant farm worker
• Family of 5 lives in a 2-bedroom trailer
• Patient works full-time as a seamstress in a small, family-owned business
• Smokes 2 ppd (since age 14) and drinks 2 beers most evenings
• Has "never used illegal drugs of any kind"
• Rarely exercises and admits to trying various fad diets for weight loss but with little
success; has given up trying to lose weight and now eats a diet rich in fats and refined
History of Present Illness
C.B. is a significantly overweight, 48-year-old woman from the Winnebago Indian tribe who
had high blood sugar and cholesterol levels three years ago but did not follow up with a clin-
ical diagnostic work-up. She had participated in the state's annual health screening program
and noticed that her fasting blood sugar was 141 and her cholesterol was 225. However, she
felt "perfectly fine at the time" and could not afford any more medications. Except for a num-
ber of "female infections," she has felt fine until recently.
Today,
sugars
presents to the Indian Hospital general practitioner complaining that her left
foot has been weak and numb for nearly three weeks and that the foot is difficult to flex. She
denies any other weakness or numbness at this time. However, she reports that she has been
very thirsty lately and gets up more often at night to urinate. She has attributed these symp-
toms to the extremely warm weather and drinking more water to keep hydrated. She has
gained a total of 65 pounds since her last pregnancy 14 years ago, 15 pounds in the last
6 months alone.
Review of Systems
General
Admits to recent onset of fatigue
HEENT
Past Medical History
• Seasonal allergic rhinitis (since her early 20s)
• Breast biopsy positive for fibroadenoma at age 30
• Gestational diabetes with fourth child 14 years ago
Morning sickness with all four pregnancies
• HTN x 10 years
• Moderate-to-severe osteoarthritis involving hands and knees x 4 years
• Multiple yeast infections during the past 3 years that she has self-treated with OTC anti-
fungal creams and salt baths
• Occasional constipation
Has awakened on several occasions with blurred vision and dizziness or lightheadedness
upon standing; denies vertigo, head trauma, ear pain, ringing sensations in the ears, diffi-
culty swallowing, and pain with swallowing
Cardiac
Denies chest pain, palpitations, and difficulty breathing while lying down
Lungs
Denies cough, shortness of breath, and wheezing
258
Expert Solution
This question has been solved!
Explore an expertly crafted, step-by-step solution for a thorough understanding of key concepts.

This is a popular solution!

Trending now
This is a popular solution!

Step by step
Solved in 3 steps

Recommended textbooks for you
Surgical Tech For Surgical Tech Pos Care
Health & Nutrition
ISBN:
9781337648868
Author:
Association
Publisher:
Cengage
Surgical Tech For Surgical Tech Pos Care
Health & Nutrition
ISBN:
9781337648868
Author:
Association
Publisher:
Cengage