
Videos
The Stealth Invader
Tim is often seen walking around campus, hanging out at the coffee shop, laughing with his friends, and, as he puts it, “investing time with the ladies.” Tim started smoking in high school and has never tried to kick the habit. He jokes about the “smoker’s cough” that has punctuated his conversations over the summer and start of the fall semester. Recently, the cough has been getting worse, his throat is scratchy, his head hurts, and he is tired all the time. Tim wonders if he has some long-lasting flu, though he hasn’t had a fever. He decides not to waste time with a doctor’s visit, but the cough starts keeping him up at night. In October, after a month of progressively worse coughing, he’s had enough; he heads to the campus clinic right after his morning classes.
The clinic physician notes the persistence and worsening of Tim’s cough and confirms that Tim has no fever. To rule out a bacterial infection, she orders a routine sputum culture (a test of the material coughed up from Tim’s lungs), which comes back negative. Tim is sent home with the advice to quit smoking.
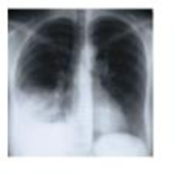
A week later, he’s back, coughing nonstop, short of breath, sweaty, and aching. A different doctor orders a chest X-ray exam and several blood tests. The X-ray film reveals fluid in Tim’s lungs, and real-time PCR confirms an infection with Mycoplasma pneumoniae, which is an atypical Gram-positive bacterium. Regular sputum microscopy doesn't detect this pathogen, which lacks cell walls and doesn’t stain well.
Mycoplasma pneumoniae infects and disrupts the mucous membranes of the lungs, invading and disrupting the epithelium. Pneumonia caused by M. pneumoniae is called “walking pneumonia” because the symptoms are often milder and come and go, making this disease different from streptococcal pneumonia. Most patients get better on their own, but not Tim. Smoke has compromised the lungs’ innate immunity. A course of an antimicrobial drug-azithromycin-clears Tim’s lungs of the bacterium within a week. Tim decides to quit smoking.
- 1. Which Toll-like receptors (TLRs) might have been involved in Tim’s innate immune response to Mycoplasma?
- 2. Why didn’t Tim’s naturally occurring interferons help clear the infection?
- 3. What structures and chemicals normally fend off lung infections?
- 4. Why didn’t Tim’s innate lung defenses operate properly?
Want to see the full answer?
Check out a sample textbook solution
Chapter 15 Solutions
EP MICROBIOLOGY:W/DISEASES BY..-MOD.ACC


- A 5-year-old child was admitted to the hospital with a history of recurrent respiratory infections. Test results revealed that the child had Kartagener’s syndrome. Explain why this syndrome leads to frequent respiratory infections.arrow_forwardKatie is a 14-year-old girl with a history of seasonal hay fever symptoms and eczema. She has been troubled recently by chest tightness, wheezing and cough. The cough is only minimally productive of whitish sputum. There is a strong family history of allergies and she received “allergy shots” when she was younger. She tells her mother that when she visits a friend’s home, where they have two cats, the symptoms seem to be much worse. Concerned about her daughter’s complaints, Katie’s mother takes her to the family clinic, where a diagnosis of asthma is eventually established. What historical factors would raise concern that Katie may have asthma? (Support Your answer with at least four possible outcomes.) What environmental factors could potentially exacerbate her condition? Include examples. (Support Your answer with at least four possible outcomes.) What are the pathophysiologic processes that are responsible for the clinical manifestations of asthma?(Support Your answer…arrow_forwardKatie is a 14-year-old girl with a history of seasonal hay fever symptoms and eczema. She has been troubled recently by chest tightness, wheezing and cough. The cough is only minimally productive of whitish sputum. There is a strong family history of allergies and she received “allergy shots” when she was younger. She tells her mother that when she visits a friend’s home, where they have two cats, the symptoms seem to be much worse. Concerned about her daughter’s complaints, Katie’s mother takes her to the family clinic, where a diagnosis of asthma is eventually established. What historical factors would raise concern that Katie may have asthma? (Support Your answer with at least four possible outcomes.) What environmental factors could potentially exacerbate her condition? Include examples. (Support Your answer with at least four possible outcomes.)arrow_forward
- Mr. Whaley is a 65-year-old man with a history of COPD who presents to his primary care provider’s (PCP) office complaining of a productive cough off and on for 2 years and shortness of breath for the last 3 days. He reports that he has had several chest colds in the last few years, but this time it won’t go away. His wife says he has been feverish for a few days, but doesn’t have a specific temperature to report. He reports smoking a pack of cigarettes a day for 25 years plus the occasional cigar. Upon further assessment, Mr. Whaley has crackles throughout the lower lobes of his lungs, with occasional expiratory wheezes throughout the lung fields. His vital signs are as follows: BP 142/86 mmHg HR 102 bpm RR 32 bpm Temp 102.3F SpO2 86% on room air The nurse locates a portable oxygen tank and places the patient on 2 lpm oxygen via nasal cannula. Based on these findings, Mr. Whaley’s PCP decides to call an ambulance to send Mr. Whaley to the Emergency Department (ED). While waiting…arrow_forwardMr. Whaley is a 65-year-old man with a history of COPD who presents to his primary care provider’s (PCP) office complaining of a productive cough off and on for 2 years and shortness of breath for the last 3 days. He reports that he has had several chest colds in the last few years, but this time it won’t go away. His wife says he has been feverish for a few days, but doesn’t have a specific temperature to report. He reports smoking a pack of cigarettes a day for 25 years plus the occasional cigar. Upon further assessment, Mr. Whaley has crackles throughout the lower lobes of his lungs, with occasional expiratory wheezes throughout the lung fields. His vital signs are as follows: BP 142/86 mmHg HR 102 bpm RR 32 bpm Temp 102.3F SpO2 86% on room air The nurse locates a portable oxygen tank and places the patient on 2 lpm oxygen via nasal cannula. Based on these findings, Mr. Whaley’s PCP decides to call an ambulance to send Mr. Whaley to the Emergency Department (ED). While waiting…arrow_forwardMr. Whaley is a 65-year-old man with a history of COPD who presents to his primary care provider’s (PCP) office complaining of a productive cough off and on for 2 years and shortness of breath for the last 3 days. He reports that he has had several chest colds in the last few years, but this time it won’t go away. His wife says he has been feverish for a few days, but doesn’t have a specific temperature to report. He reports smoking a pack of cigarettes a day for 25 years plus the occasional cigar. Upon further assessment, Mr. Whaley has crackles throughout the lower lobes of his lungs, with occasional expiratory wheezes throughout the lung fields. His vital signs are as follows: BP 142/86 mmHg HR 102 bpm RR 32 bpm Temp 102.3F SpO2 86% on room air The nurse locates a portable oxygen tank and places the patient on 2 lpm oxygen via nasal cannula. Based on these findings, Mr. Whaley’s PCP decides to call an ambulance to send Mr. Whaley to the Emergency Department (ED).…arrow_forward
- Which of the following pathogens mimic the host bilayer for transmission through the plasma membrane of human respiratory tract epithelial cells? Streptococcus pneumoinae O Legionella pneumophila O Mycoplasma pneumoniaearrow_forwardWhich of the following statements is CORRECT regarding viral infections of the upper respiratory tract?A The virus causes damage to serous cells but not ciliated cellsB Children with croup develop an expiratory stridorC The virus attaches and invades the respiratory capillariesD Secondary bacterial infections are often a complication of viral infectionsarrow_forwardThe mother of a 6-year-old child brings her daughter to the pediatrician's office because she has had a sore throat, cough, and fever for several days. She reports a fever up to 104°F that worsens at night, but seems to respond to treatment with acetaminophen. The child has not been eating or drinking well because she says, "it hurts to swallow." She is ill appearing, and does not seem interested in playing with the toys that are in the examination room. The physician notes a thick, white exudate on both of the patient's tonsils, which also seem enlarged. A throat culture and complete blood count with differential is ordered. 1) The patient's mother expresses concern about her daughter's fevers. She states that the fevers are a sign that her child is unable to fight this infection. What is a proper response to these concerns? A) It is impossible to determine exactly why she is having these fevers. Doctors call this a fever of unknown origin. B) Fevers are a natural response by the…arrow_forward
- Bacterial (e.g., S. pneumoniae) pneumonia is commonly manifested by a cough productive of sputum, whereas with atypical (e.g., Mycoplasma pneumoniae) pneumonia, the cough is usually nonproductive or absent. Explain.arrow_forwardA patient presented to the emergency room complaining of a nonproductive cough (no sputum) that had persisted for six weeks. The clinician prescribed a 7-day course of cephalosporin. After day 7 the patient returned, no better than when he started. Laboratory tests later showed the infection was caused by Mycoplasma pneumoniae. Explain why the antibiotic did not work.arrow_forwardYour 3-month-old son is taken to the emergency room because he has a fever and difficulty breathing. The child is admitted to intensive care because the doctor thinks he has a type of pneumonia whose name you do not recognize. The doctor reports that the hospital has seen a dozen pediatric cases of this pneumonia in the past week. The doctor swabs your son’s nose but says the results won’t be back for several days. In the meantime, they will give supportive therapy, including an inhaled spray, but no antibacterial drugs. The doctor feels sure the child will recover. 1. What kind of pneumonia is it? 2. Why aren’t they giving him antibacterial drugs? 3. How can the doctor be sure what’s causing the pneumonia if she doesn’t yet have test results? 4. Has the other child (a 3 years-old) been exposed to the infection?arrow_forward
 Medical Terminology for Health Professions, Spira...Health & NutritionISBN:9781305634350Author:Ann Ehrlich, Carol L. Schroeder, Laura Ehrlich, Katrina A. SchroederPublisher:Cengage Learning
Medical Terminology for Health Professions, Spira...Health & NutritionISBN:9781305634350Author:Ann Ehrlich, Carol L. Schroeder, Laura Ehrlich, Katrina A. SchroederPublisher:Cengage Learning