Pearson eText Human Physiology: An Integrated Approach -- Instant Access (Pearson+)
8th Edition
ISBN: 9780135212905
Author: Dee Silverthorn
Publisher: PEARSON+
expand_more
expand_more
format_list_bulleted
Videos
Textbook Question
Chapter 20, Problem 33RQ
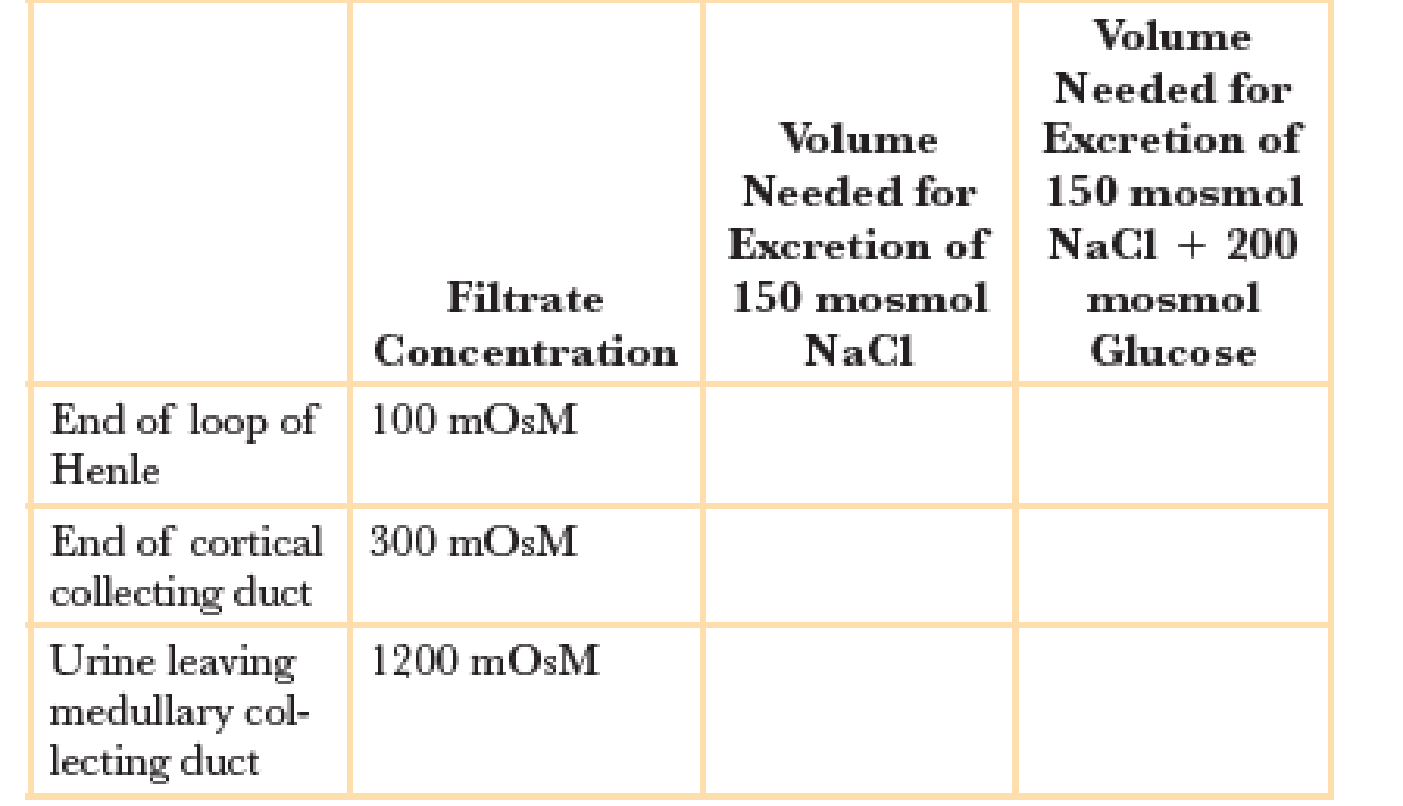
Osmotic diuresis refers to the loss of additional water in urine as a result of unreabsorbed solutes. To see what difference unreabsorbed solutes make, calculate the volumes of filtrate that would be needed for excretion of 150 milliosmoles of NaCl. Then repeat the calculation for a diabetic who is excreting the same 150 mosmol NaCl plus 200 mosmol unreabsorbed glucose.
Expert Solution & Answer
Want to see the full answer?
Check out a sample textbook solution
Students have asked these similar questions
Diabetes insipidus (DI) is a condition where the action of antidiuretic hormone (vasopressin) is inhibited. If normal urine concentration is 300 mOsm/L, what would you expect the urine concentration to be of a patient with DI?
A 28-year-old man has a fasting serum glucose concentration of 140 mg/dL and a glomerular filtration rate of 125 ml/min. The renal transport maximum for glucose in this patient is 300 mg/min. Which of the following best represents the rate of urinary glucose excretion (in mg/min) in this man?
(A) 0
(B) 100
(C) 200
(D) 300
(E) 400
Say someone has a blood glucose level of 245
mg/dl. Which statement below would be
correct?
O They would exhibit glycosuria because the
transport maximum of glucose has been
exceeded.
O They would exhibit glycosuria because of
decreased osmosis in the urine collecting duct.
O They would not exhibit glycosuria because the
transport maximum of glucose has been
exceeded.
O They would not exhibit glycosuria because of
decreased osmosis in the urine collecting duct.
Chapter 20 Solutions
Pearson eText Human Physiology: An Integrated Approach -- Instant Access (Pearson+)
Ch. 20.2 - Does the apical membrane of a collecting duct cell...Ch. 20.2 - Prob. 2CCCh. 20.2 - A scientist monitoring the activity of...Ch. 20.2 - If vasopressin increases water reabsorption by the...Ch. 20.2 - Experiments suggest that there are peripheral...Ch. 20.2 - Prob. 6CCCh. 20.2 - Prob. 7CCCh. 20.3 - In Figure 20.9b, what forces cause Na+ and K+ to...Ch. 20.3 - Prob. 9CCCh. 20.3 - Laboratory values for ions may be reported as...
Ch. 20.3 - A man comes to the doctor with high blood...Ch. 20.3 - Map the pathways through which elevated renin...Ch. 20.3 - Why is it more efficient to put ACE in the...Ch. 20.5 - Incorporate the thirst reflex into Figure 20.8.Ch. 20.6 - Map the pathway that begins with renal artery...Ch. 20.7 - CO2+H2OH++HCO3(6) In equation 6, the amount of...Ch. 20.7 - Why is ATP required for H+ secretion by the H+-K+...Ch. 20.7 - In hypokalemia, the intercalated cells of the...Ch. 20 - What is an electrolyte? Name five electrolytes...Ch. 20 - Prob. 2RQCh. 20 - Prob. 3RQCh. 20 - List the receptors that regulate osmolarity, blood...Ch. 20 - How do the two limbs of the loop of Henle differ...Ch. 20 - Prob. 6RQCh. 20 - Prob. 7RQCh. 20 - Prob. 8RQCh. 20 - Write out the words for the following...Ch. 20 - Prob. 10RQCh. 20 - Prob. 11RQCh. 20 - Prob. 12RQCh. 20 - Prob. 13RQCh. 20 - Prob. 14RQCh. 20 - Prob. 15RQCh. 20 - When ventilation increases, what happens to...Ch. 20 - Prob. 17RQCh. 20 - Figures 20.15 and 20.18a show the respiratory and...Ch. 20 - Explain how the loop of Henle and vasa recta work...Ch. 20 - Prob. 20RQCh. 20 - Prob. 21RQCh. 20 - Name the four main compensatory mechanisms for...Ch. 20 - Prob. 23RQCh. 20 - Compare and contrast the terms in each set: a....Ch. 20 - Prob. 25RQCh. 20 - Prob. 26RQCh. 20 - Prob. 27RQCh. 20 - Hannah, a 31-year-old woman, decided to have...Ch. 20 - Prob. 29RQCh. 20 - Prob. 30RQCh. 20 - The Henderson-Hasselbalch equation is a...Ch. 20 - Hyperglycemia in a diabetic patient leads to...Ch. 20 - Osmotic diuresis refers to the loss of additional...
Knowledge Booster


Learn more about
Need a deep-dive on the concept behind this application? Look no further. Learn more about this topic, biology and related others by exploring similar questions and additional content below.Similar questions
- Table 3. Serum creatinine values at admission and after 12h Admission +12h SCR(mg/dL) 1.55 1.42 Using the “MDRD” (Modification of Diet in Renal Disease) equation for estimating glomerularfiltration, provided below, and the data available in the above table, calculate the patient's (a 34 year old white male) estimated glomerularfiltration rate (eGFR) at admission and 12h after admission.MDRD GFR Equation (mL/min/1.73 m2)= 175 × (Scr)-1.154 × (Age)-0.203 × (0.742 if female) × (1.212 if African American)Based on your calculated values, state whether LF’s function is normal or abnormal?Previous research suggests that patients with asthma have an increased risk for chronic kidneydisease, but the mechanisms underlying this increased risk are poorly understood. Propose one potential mechanism by which asthma might impair kidney function, and discuss how this dysfunction may impair thebody’s ability to respond to respiratory alkalosisarrow_forwardRenin is secreted in response to hypovolemia or to an increase in the osmolality of the blood. Provide three possible mechanisms by which these conditions may stimulate rennin secretion. What are the consequences of increased rennin secretion that lead to increased aldosterone secretion? Present this sequence of events. Why are angiotensin converting enzyme inhibitors (ACEIs) used as a common therapy for hypertension? How do they influence blood pressure? Are plasma levels of renin elevated or depressed in a patient with Conn’s disease? Why?arrow_forwardExplain the mechanism how furosemide affects kidney tubules. How does this affect K+ balance? How different is the mechanism of thiazide affect urine production? Describe the process of acid-base regulation in human body.arrow_forward
- Acetazolamide is a diuretic that blocks the activity of the enzyme carbonic anhydrase inside kidney tubule cells. This blockage prevents theformation of carbonic acid from CO2 and water. Normally, carbonicacid dissociates to form H+ and HCO3−, and the H+ is exchanged forNa+ from the urine. Blocking the formation of H+ in the tubule cellsblocks Na+ reabsorption, thus inhibiting water reabsorption andproducing the diuretic effect. With this information in mind, what effectdoes acetazolamide have on blood pH, urine pH, and respiratory rate?arrow_forwardAll of the following are true about glucose recovery from the tubule fluid, except (choose the incorrect statement): A. All filtered glucose is released in the PCT unless plasma glucose abnormally high B. It is reabsorbed by coupling with Na+ recovery via a sodium glucose cotransporter C. Glucose recovery is made possible by low intracellular Na+ concentrations created by the NaK pump D. The CD recovers any glucose that is not reabsorbed by the PCT nephron loop and DCT this is not and will not be gradedarrow_forwardAtrial Natriuretic Peptide helps to reduce overall blood pressure in a variety of ways. One way is by increasing Glomerular Filtration Rate. a. Why/how would increasing GFR cause decreased blood pressure? b. To increase GFR, would Atrial Natriuretic Peptide cause constriction or dilation of afferent arterioles at the kidneys? The efferent arterioles?arrow_forward
- The presence of either protein or glucose in a urinalysis is abnormal, but these two molecules end up in the urine for different reasons. For each of these molecules, briefly describe where in the urine production process (i.e., glomerular filtration, tubular reabsorption or tubular secretion) the problem occurs, and why it might happen.arrow_forwardWhy is this statement false? Without the renal medullar osmotic gradient, you would not be able to raise the concentration of urine above 1200 mOsmarrow_forwardOne model of the glomerular membrane is a microporous membrane in which right cylindrical pores penetrate all the way through the membrane. Assume that the pores have a length of 50 nm and a radius of 3.5 nm. The viscosity of plasma is 0.002 Pa s. The average hydrostatic pressure in the glomerulus is 60 mm Hg, hydrostatic pressure in Bowman's space is 20 mm Hg and the average oncotic pressure of glomerular capillary blood is 28 mm Hg. A. Calculate the flow through a single pore assuming laminar flow (use the Poiseuille flow equation) B. How many pores would there have to be to produce a normal GFR? C. If the total aggregate area of the kidneys for filtration is 1.5 m2, what is the density of the pores (number of pores per unit area)? D. What fraction of the area is present as pores?arrow_forward
- A uremic patient has a urine output of 1.8 L/24 h and an average creatinine concentration of 2.2 mg/dL. What is the creatinine clearance? How would you adjust the dose of a drug normally given at 20 mg/kg every 6 hours in this patient (assume the urine creatinine concentration is 0.1 mg/mL and creatinine clearance is 100 mL/min)?arrow_forward1. 3 of the following are true of the Renin Angiotensin Aldosterone System (RAAS) A. The JG cells are located at the distal collecting tubule B. The Juxtaglomerular cells (JG cells) are modified smooth muscles in the afferent arteriole C. The Macula densa detects osmolality of the filtrate D. The Macula densa is made up of tall columnar cells 2. 2 of the following are true of the RAAS responding to a decrease in Na in the filtrate A. Macula densa detects the decrease in osmolality B. JG cells are stimulated by Macula densa through tight junctions C. Aldosterone stimulates principal cells of collecting tubule to reabsorb water D. Aldosterone reabsorbs Na and by osmotic forces increase fluid in the extracellular compartment 3. 2 of the following are true of the loop of Henle A. Descending thick limb is also called the pars recta of the proximal tubule B. The function of the descending thick limb is similar to the distal convoluted tubule C. Cells of the descending thin limb are very…arrow_forwardThe renal handling of a novel drug is being studied. When the drug is present in the blood, it is filtered into the Bowman’s capsule and secreted via transport proteins in the renal tubules, but it is NOT reabsorbed. The lines on the following graph represent filtration, secretion and excretion rates of this drug at various plasma concentrations. For the three lines shown (labeled A-C) identify which line represents filtration, which line represents secretion, and which line represents excretion Explain how you determined this.arrow_forward
arrow_back_ios
SEE MORE QUESTIONS
arrow_forward_ios
Recommended textbooks for you
 Human Physiology: From Cells to Systems (MindTap ...BiologyISBN:9781285866932Author:Lauralee SherwoodPublisher:Cengage Learning
Human Physiology: From Cells to Systems (MindTap ...BiologyISBN:9781285866932Author:Lauralee SherwoodPublisher:Cengage Learning
Human Physiology: From Cells to Systems (MindTap ...
Biology
ISBN:9781285866932
Author:Lauralee Sherwood
Publisher:Cengage Learning
Excretory System; Author: Amoeba Sisters;https://www.youtube.com/watch?v=q5qaGHfdmYM;License: Standard youtube license