Concept explainers
Videos
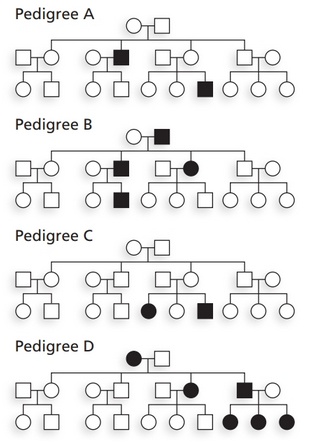
For each pedigree shown,
a. Identify which simple pattern of hereditary trans-mission (autosomal dominant, autosomal recessive, X-linked dominant, or X-linked recessive) is most likely to have occurred. Give genotypes for individuals involved in transmitting the trait.
b. Determine which other pattern(s) of transmission is/are possible. For each possible mode of transmission, specify the genotypes necessary for transmission to occur.
c. Identify which pattern(s) of transmission is/are impossible. Specify why transmission is impossible.

Learn your wayIncludes step-by-step video

Chapter 3 Solutions
Genetic Analysis: An Integrated Approach (2nd Edition)
Additional Science Textbook Solutions
Campbell Biology in Focus
Human Anatomy & Physiology
Concepts of Genetics (12th Edition)
Campbell Biology: Concepts & Connections (9th Edition)
Laboratory Experiments in Microbiology (12th Edition) (What's New in Microbiology)
Brock Biology of Microorganisms (15th Edition)


- Familial retinoblastoma, a rare autosomal dominant defect, arose in a large family that had no prior history of the disease. Consider the following pedigree (the darkly colored symbols represent affected individuals): a. Circle the individual(s) in which the mutation most likely occurred. b. Is the person who is the source of the mutation affected by retinoblastoma? Justify your answer. c. Assuming that the mutant allele is fully penetrant, what is the chance that an affected individual will have an affected child?arrow_forwardExamine the following pedigrees. Which is the most likely mode of inheritance of each disorder? (a) autosomal recessive (b) autosomal dominant (c) X-linked recessive (d) a, b, or c (e) a or c 10.arrow_forwardA couple was referred for genetic counseling because they wanted to know the chances of having a child with dwarfism. Both the man and the woman had achondroplasia (MIM 100800), the most common form of short-limbed dwarfism. The couple knew that this condition is inherited as an autosomal dominant trait, but they were unsure what kind of physical manifestations a child would have if it inherited both mutant alleles. They were each heterozygous for the FGFR3 (MIM 134934) allele that causes achondroplasia. Normally, the protein encoded by this gene interacts with growth factors outside the cell and receives signals that control growth and development. In achrodroplasia, a mutation alters the activity of the receptor, resulting in a characteristic form of dwarfism. Because both the normal and mutant forms of the FGFR3 protein act before birth, no treatment for achrondroplasia is available. The parents each carry one normal allele and one mutant allele of FGRF3, and they wanted information on their chances of having a homozygous child. The counsellor briefly reviewed the phenotypic features of individuals with achondroplasia. These include facial features (large head with prominent forehead; small, flat nasal bridge; and prominent jaw), very short stature, and shortening of the arms and legs. Physical examination and skeletal X-ray films are used to diagnose this condition. Final adult height is approximately 4 feet. Because achondroplasia is an autosomal dominant condition, a heterozygote has a 1-in-2, or 50%, chance of passing this trait to his or her offspring. However, about 75% of those with achondroplasia have parents of average size who do not carry the mutant allele. In these cases, achondroplasia is due to a new mutation. In the couple being counseled, each individual is heterozygous, and they are at risk for having a homozygous child with two copies of the mutated gene. Infants with homozygous achondroplasia are either stillborn or die shortly after birth. The counselor recommended prenatal diagnosis via ultrasounds at various stages of development. In addition, a DNA test is available to detect the homozygous condition prenatally. What if the couple wanted prenatal testing so that a normal fetus could be aborted?arrow_forward
- A couple was referred for genetic counseling because they wanted to know the chances of having a child with dwarfism. Both the man and the woman had achondroplasia (MIM 100800), the most common form of short-limbed dwarfism. The couple knew that this condition is inherited as an autosomal dominant trait, but they were unsure what kind of physical manifestations a child would have if it inherited both mutant alleles. They were each heterozygous for the FGFR3 (MIM 134934) allele that causes achondroplasia. Normally, the protein encoded by this gene interacts with growth factors outside the cell and receives signals that control growth and development. In achrodroplasia, a mutation alters the activity of the receptor, resulting in a characteristic form of dwarfism. Because both the normal and mutant forms of the FGFR3 protein act before birth, no treatment for achrondroplasia is available. The parents each carry one normal allele and one mutant allele of FGRF3, and they wanted information on their chances of having a homozygous child. The counsellor briefly reviewed the phenotypic features of individuals with achondroplasia. These include facial features (large head with prominent forehead; small, flat nasal bridge; and prominent jaw), very short stature, and shortening of the arms and legs. Physical examination and skeletal X-ray films are used to diagnose this condition. Final adult height is approximately 4 feet. Because achondroplasia is an autosomal dominant condition, a heterozygote has a 1-in-2, or 50%, chance of passing this trait to his or her offspring. However, about 75% of those with achondroplasia have parents of average size who do not carry the mutant allele. In these cases, achondroplasia is due to a new mutation. In the couple being counseled, each individual is heterozygous, and they are at risk for having a homozygous child with two copies of the mutated gene. Infants with homozygous achondroplasia are either stillborn or die shortly after birth. The counselor recommended prenatal diagnosis via ultrasounds at various stages of development. In addition, a DNA test is available to detect the homozygous condition prenatally. What is the chance that this couple will have a child with two copies of the dominant mutant gene? What is the chance that the child will have normal height?arrow_forwardA couple was referred for genetic counseling because they wanted to know the chances of having a child with dwarfism. Both the man and the woman had achondroplasia (MIM 100800), the most common form of short-limbed dwarfism. The couple knew that this condition is inherited as an autosomal dominant trait, but they were unsure what kind of physical manifestations a child would have if it inherited both mutant alleles. They were each heterozygous for the FGFR3 (MIM 134934) allele that causes achondroplasia. Normally, the protein encoded by this gene interacts with growth factors outside the cell and receives signals that control growth and development. In achrodroplasia, a mutation alters the activity of the receptor, resulting in a characteristic form of dwarfism. Because both the normal and mutant forms of the FGFR3 protein act before birth, no treatment for achrondroplasia is available. The parents each carry one normal allele and one mutant allele of FGRF3, and they wanted information on their chances of having a homozygous child. The counsellor briefly reviewed the phenotypic features of individuals with achondroplasia. These include facial features (large head with prominent forehead; small, flat nasal bridge; and prominent jaw), very short stature, and shortening of the arms and legs. Physical examination and skeletal X-ray films are used to diagnose this condition. Final adult height is approximately 4 feet. Because achondroplasia is an autosomal dominant condition, a heterozygote has a 1-in-2, or 50%, chance of passing this trait to his or her offspring. However, about 75% of those with achondroplasia have parents of average size who do not carry the mutant allele. In these cases, achondroplasia is due to a new mutation. In the couple being counseled, each individual is heterozygous, and they are at risk for having a homozygous child with two copies of the mutated gene. Infants with homozygous achondroplasia are either stillborn or die shortly after birth. The counselor recommended prenatal diagnosis via ultrasounds at various stages of development. In addition, a DNA test is available to detect the homozygous condition prenatally. Should the parents be concerned about the heterozygous condition as well as the homozygous mutant condition?arrow_forwardA man who has color blindness and type O blood has children with a woman who has normal color vision and type AB blood. The woman’s father had color blindness. Color blindness is determined by an X-linked gene, and blood type is determined by an autosomal gene. a. What are the genotypes of the man and the woman? b. What proportion of their children will have color blindness and type B blood? c. What proportion of their children will have color blindness and type A blood? d. What proportion of their children will be color blind and have type AB blood?arrow_forward
- A mother is heterozygous for the X-linked gene for colorblindness and also heterozygous for the autosomal inherited sickle cell anemia. She is married to a man who can see color normally and who is heterozygous for sickle cell trait. Using b (colorblind), B (normal color), S (normal hemoglobin), s (sickle cell), answer the following: a. What are the genotypes of the parents? b: What is the probability of having a child who is both color blind and has sickle cell anemia?arrow_forwardNote: Don't copy from internet, Also answer correctly in terms of diploid, hemizygous, and carrier!! Thanks Explain why genetic disorders caused by recessive alleles of X-linked genes appear more frequently in males than in females? In your explanation, please include explanations of the following terms: diploid, hemizygous, carrier.arrow_forwardI will be adding two questions here because I asked two of the same questions twice by accident earlier. A man and a woman do not have hemophilioa, but the womans father did. (Hemophilia is X-linked recessive). a) What is the probability that they will have a child with hemophilia? b) Is it possible for any of their daughters to be affected? Explain. A cross between a horse homozygous for red hair and a horse homozygous for white hair results in offspring with the coat colour called roan. When you look at the fur of the roan offspring you see both red and white hairs. What type of inheritance best explains this? a) blending inheritance b)codominance c)incomplete codominance d)multiple allelesarrow_forward
- Now assume that the pedigree shown in question 1 shows the inheritance of a rare genetic disease. a) The disease is most likely autosomal dominant b) The disease is most likely autosomal recessive c) The disease is equally likely to be either autosomal dominant or autosomal recessive, but cannot be x-linked d) Cannot be determined from the information givenarrow_forwardPropose the most likely mode of inheritance (autosomal dominant, autosomal recessive, or X-linked recessive) for the following pedigrees. Affected individuals are shown with filled (black)symbols.arrow_forwardWhat genetic criteria distinguish a case of extranuclear inheritance from (a) a case of Mendelian autosomal inheritance; (b) a case of X-linked inheritance?arrow_forward
 Human Heredity: Principles and Issues (MindTap Co...BiologyISBN:9781305251052Author:Michael CummingsPublisher:Cengage Learning
Human Heredity: Principles and Issues (MindTap Co...BiologyISBN:9781305251052Author:Michael CummingsPublisher:Cengage Learning Biology (MindTap Course List)BiologyISBN:9781337392938Author:Eldra Solomon, Charles Martin, Diana W. Martin, Linda R. BergPublisher:Cengage Learning
Biology (MindTap Course List)BiologyISBN:9781337392938Author:Eldra Solomon, Charles Martin, Diana W. Martin, Linda R. BergPublisher:Cengage Learning